
")
GYNECOMASTIA SURGERY IN DUBAI
Man-Boobs Are More Common Than You Think. And More Fixable Than You Know.
Let me be straight with you — gynecomastia is one of the most common things I see in my clinic. And it’s also one of the most under-talked about, because most men suffer in silence rather than ask for help.
If you avoid tight t-shirts, think twice before taking your shirt off at the beach, or find yourself checking your chest in the mirror before you leave the house — you already know what I’m talking about.
The good news? This is one of the most straightforward procedures I perform. It’s done as a day case. You go home the same day. And the results are immediate.
GYNECOMASTIA
Two Types of Gynecomastia — And Why It Matters
Gynecomastia isn’t one thing. There are two very different types, and knowing which one you have changes everything about how we approach it.
Type 1 — Puberty-Related Gynecomastia
This is the classic man-boobs presentation. It usually starts during teenage years when hormones are all over the place, and for many men it never fully goes away. What you’re dealing with here is a combination of fatty tissue and glandular tissue — it’s why no amount of bench pressing or cutting calories ever really fixes it. You can lose weight, get lean, build a great chest — and still have that fullness or puffiness that just won’t budge.
For these patients, I perform liposuction of the chest and the axilla — that’s the armpit area — alongside gland removal. The reason I include the axilla is important: gynecomastia tissue often extends into that area, and if you only treat the chest, you can still be left with a visible fullness when you raise your arms or wear a fitted shirt. Treating both gives you a result that looks right from every angle.
This isn’t just about removing a gland. It’s about shaping the entire chest — the pectoral border, the sternal line, the lateral sweep — so the final result looks genuinely masculine and athletic, not just flat.
Type 2 — Anabolic Steroid-Related Gynecomastia
This one is extremely common among my bodybuilder patients, and I want to address it directly because I understand this world from the inside.
Anabolic steroids — testosterone, masteron, primobolan, Anavar — and even some popular gym supplements like Total War — can trigger glandular growth in the chest. It happens because these compounds affect your estrogen-to-testosterone ratio, and the breast gland tissue responds.
I hear it all the time in my clinic. Patients come in and say: “Doc, I have gyno. It’s very visible in tight clothes or white t-shirts and I hate it.”
When I examine these patients, what I typically find is a firm lump or swelling directly under the nipple — sometimes both sides, sometimes one side more than the other. The classic puffy nipple look. There’s usually very little fat involved — it’s almost entirely gland.
For these patients, gland removal alone is usually all that’s needed. No liposuction required in most cases. A small, discreet incision at the edge of the areola, the gland comes out, and the chest is flat.
")
Why Choose Dr. Ganatra for Gynecomastia Surgery in Dubai?
I’m a bodybuilder myself — I genuinely understand both types of patient.
I know what it’s like to care deeply about how your chest looks. I know the difference between a chest that looks athletic and one that just looks flat. I know what anabolic steroid use does to the body because I understand that world. My patients don’t have to explain themselves — I already get it.
I don’t just remove the gland. I shape the chest.
For puberty-related cases, I treat the chest and axilla together as one unit — liposuction plus gland removal — so the result looks proportionate and complete from every angle. For steroid-related cases, I remove exactly what needs to go and nothing more, preserving the tissue underneath the areola to prevent the “sunken” or crater look that can happen with over-resection.
The scars are as discreet as I can make them.
The gland comes out through a small half-moon incision right at the edge of the areola, where the scar hides in the natural color change of the skin. Liposuction access points are tiny — 3 to 4mm — and placed in natural creases. Most patients tell me they can barely find them a few months later.
I have real experience with complex and revision cases.
Steroid-related gynecomastia can be dense and fibrous. Revision cases — where someone has had surgery elsewhere and been left with a crater, asymmetry, or residual gland — require a different level of skill. This is work I do regularly.
I’ll be honest about whether the gland might come back.
If you’re still using the compounds that caused it, the gland can regrow after surgery. I’ll have that conversation with you openly, without judgment, so you can make an informed decision about timing and approach.
- Safety-first protocols: Hospital setting, anesthetist clearance, controlled tumescent planning, thermal-energy safeguards, and VTE-risk reduction.
- Thoughtful workup & honest guidance: When appropriate, endocrine review and lifestyle factors addressed; clear discussion of grade, expectations, and whether skin tightening or staging is wiser.
- Recovery optimized for performance: Structured compression vest schedule, lymphatic drainage, silicone/scar therapy, and a phased return-to-gym plan tailored to lifters.
- Consistent, natural outcomes: A flatter, firmer chest that fits your frame—in and out of a T-shirt.

Are You a Good Candidate?
You’re likely a great candidate if:
- You have puffy nipples or a lump under the nipple that doesn’t change with diet or training
- You have chest fullness or breast-like tissue that persists regardless of your body fat
- Your weight has been stable and you’re in good overall health
- You’re not a smoker, or you’re willing to stop ahead of surgery
- You have realistic expectations — you want a flat, masculine chest, not a miracle
One important note: if you’re currently using anabolic steroids or supplements that may be contributing to the gynecomastia, we need to discuss timing. Operating while the trigger is still active increases the risk of the gland regrowing. I’ll guide you on this during the consultation — no judgment, just practical advice.
")
What Happens Before Your Surgery
- A proper examination first: I need to feel the tissue to determine what we’re actually dealing with — fatty, glandular, or a mix of both. This physical assessment determines the surgical approach. No two cases are planned from a photo alone.
- A clear explanation of your type and your plan: I’ll tell you exactly which type of gynecomastia you have, what the procedure involves, and what the realistic result looks like. You’ll leave the consultation knowing precisely what’s happening and why.
- Medical clearance: Routine bloodwork. In some cases — particularly where there’s a hormonal component — I may recommend an endocrine review before proceeding.
- Clinical photos and measurements: Standardized and fully confidential. Essential for planning and for comparing results afterward.
- Full consent discussion: Every realistic outcome, every risk, the recovery timeline — explained clearly before you sign anything.
- An anesthesiologist meeting: Every patient meets the anesthesiologist before the procedure. Non-negotiable at my facility.
What Is a Gynecomastia Surgery?
Step 1: Marking
Markings are made while you’re standing — mapping the gland position, the chest contours, and the liposuction zones where applicable. This is where the surgical plan is translated onto your body.
Step 2: Liposuction of the Chest and Axilla (puberty-related cases)
VASER liposuction is used to remove the fatty component and loosen the glandular attachments, while also shaping the chest and clearing the axilla. This step is what gives the result its athletic, proportionate look — not just flat, but shaped.
Step 3: Gland Removal
Through a small incision at the edge of the areola, the firm glandular disc is carefully removed. I always leave a thin layer of tissue under the areola to support the nipple and prevent the sunken appearance that comes from over-resection. Precision here is everything.
Step 4: Symmetry Check and Closure
Both sides are assessed and blended before closing. Incisions are closed with fine, dissolvable sutures. A compression vest is applied immediately.
Anesthesia Options
Both procedures are performed as day cases — you come in, the surgery is done, and you go home the same day. Anesthesia options are flexible depending on what you’re comfortable with:
- Local anesthesia — for straightforward cases, awake but completely numb
- Local anesthesia with sedation — you’re relaxed and drowsy but not fully under
- General anesthesia — for patients who are anxious about the procedure or prefer to be completely asleep
I never judge a patient for wanting general anesthesia. Some people simply don’t want to be aware of anything happening, and that’s completely valid. We make it work either way.

Recovery — What to Expect
Gynecomastia is one of the easier recoveries in my practice — most patients are surprised by how manageable it is.
- Days 1–3: Mild swelling and tightness. Compression vest worn full time. Most patients are comfortable and moving around normally within 24–48 hours.
- Week 1: Light movement encouraged. Drains, if used, are removed. You’ll already see a significant difference in chest shape even through the early swelling.
- Weeks 2–3: Most patients are back to desk work and light daily activity.
- Weeks 4–6: Gradual return to the gym. Upper body and chest work comes back last — but it comes back.
- Month 3: Final contour is clear. Swelling has fully settled and the chest looks the way it’s going to look.
Aftercare includes:
- Compression vest for 4–6 weeks
- Lymphatic drainage sessions
- Silicone scar therapy for the areola incision
- Regular follow-up visits
And as with all my patients who train — you’ll get a customized return-to-gym and diet plan. I know the question you’re going to ask me is “when can I train chest again?” I’ll give you a real, specific answer.

Can You Combine Gynecomastia With Other Procedures?
Yes — and for my bodybuilder patients especially, combining makes a lot of sense. Common combinations include:
- HD Liposuction of the abdomen and flanks — for a complete athletic upper body transformation
- J-Plasma — in cases where there’s skin laxity alongside the gynecomastia
- Arm or back liposuction — for full upper body sculpting in one session
GYNECOMASTIA
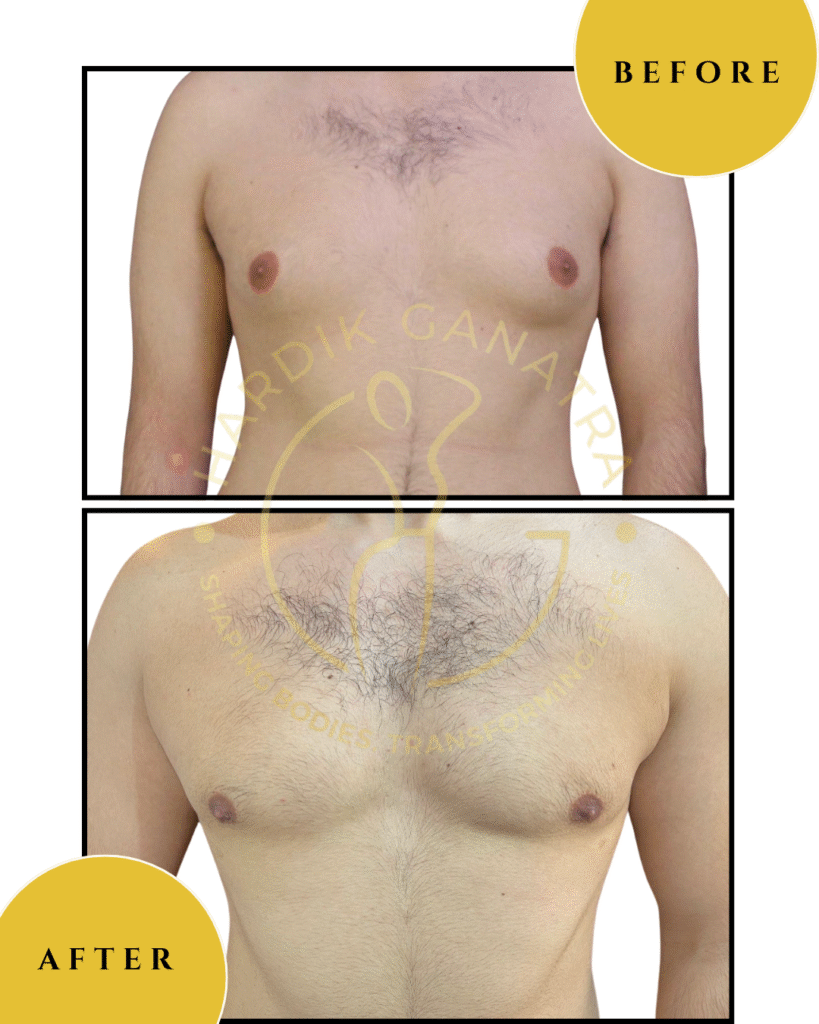
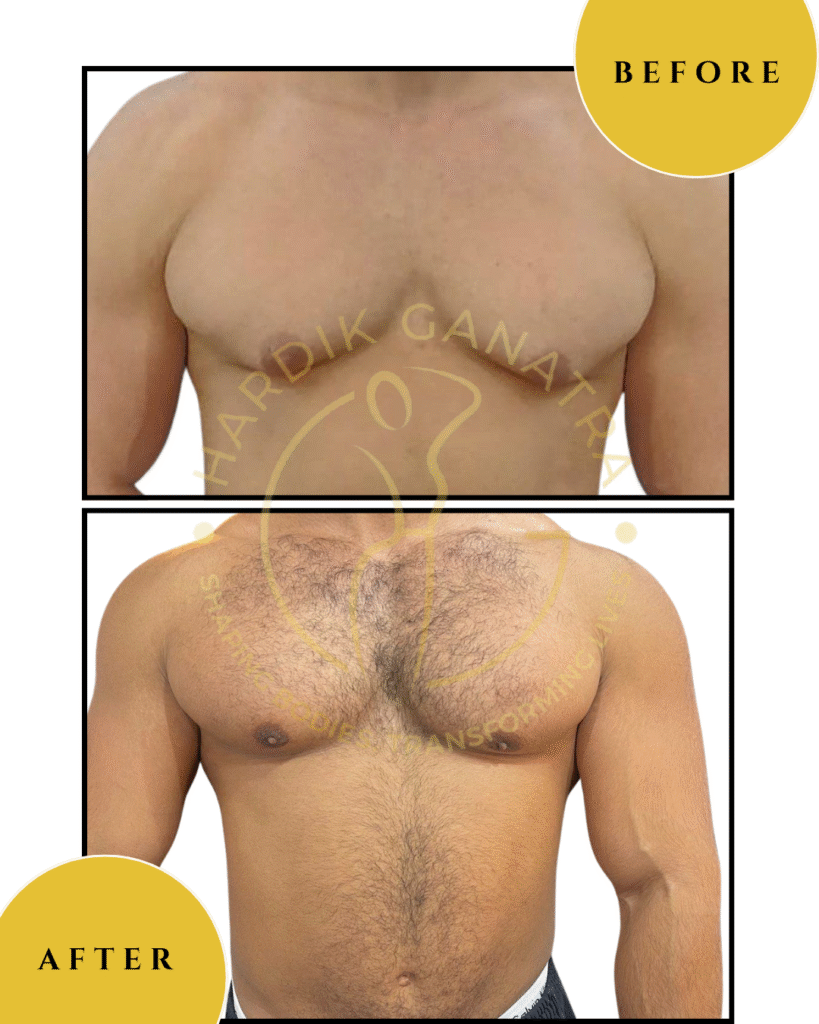
Before & After
Each transformation under Dr. Hardik Ganatra’s care is designed to look balanced, masculine, and natural.









What OUR Patients are saying ?
“For the first time, I could wear a T-shirt without overthinking.”
“I had struggled with gynecomastia since my teenage years. No amount of gym or diet could fix it — it affected my confidence every single day. Dr. Ganatra was understanding from the first consultation, and the surgery was seamless. The results look natural, the scars are barely visible, and I finally feel comfortable in my own skin.”
— A.R., 27, Dubai
“It changed more than how I look — it changed how I carry myself.”
“I used to avoid beaches, tight shirts, even mirrors. After my gynecomastia correction with Dr. Ganatra, I realized how much this held me back. The procedure was smooth, recovery was fast, and the confidence it gave me is priceless. It’s not just a cosmetic change — it’s freedom.”
— V.S., 31, India
GYNECOMASTIA Frequently Asked Questions
1. Will the gym fix it?
Honest answer — no, if there’s a gland involved. You can reduce the fat component by getting lean, but glandular tissue doesn’t respond to training or diet. Many of my patients are already very fit and lean when they come to see me. That’s actually what makes it more visible — less fat around it means the gland stands out more.
2. Can it come back after surgery?
The gland that’s removed is gone. But if the trigger is still active — ongoing steroid or supplement use, for example — new glandular tissue can potentially regrow. We’ll discuss this honestly during your consultation so the timing of surgery makes sense for your situation.
3. Will the nipple look sunken or flat after surgery?
Not with proper technique. I deliberately leave a thin layer of tissue beneath the areola specifically to prevent this. Over-resection is one of the most common mistakes in gynecomastia surgery — it’s something I’m very careful to avoid.
4. Is it just a lump or is it all fat?
This is actually a great question to ask before surgery, because the answer determines the approach. A firm disc or lump under the nipple is glandular — liposuction alone won’t remove it and a gland excision is needed. Softer, more diffuse chest fullness is more likely fatty. Most cases are a combination of both, which is why a proper physical examination is essential before planning anything.
5. Do I need to stop steroids before surgery?
This is something we’ll discuss in detail. In general, operating while the hormonal trigger is still active isn’t ideal — but the specifics depend on your situation. I’ll give you practical, honest guidance without any judgment.
6. Is it painful?
Most patients describe the discomfort as very manageable — tightness and mild soreness rather than significant pain. Prescribed pain control handles the first few days comfortably.
7. Will I need drains?
Not always. In many cases, a proper compression protocol is sufficient. For more extensive dissections, a small drain may be placed for 24–48 hours. Your individual plan determines this.
8. How much does gynecomastia surgery cost in Dubai?
The cost depends on the type — gland removal only vs. liposuction plus gland removal, whether the axilla is included, anesthesia type, and facility time. You’ll receive a personalized quote after your consultation.